Click here for updated 2022 Myth vs Fact sheet for SB88.
“It appears that the electorate doesn’t care that much about it, no matter what the polling says.” – spokesperson for assisted suicide group in Connecticut, January 2015
It’s about radical autonomy, not pain.
The top reasons for a deadly prescription in Oregon is fear of losing autonomy (91.5%), of being less able to engage in activities (88.7%) and loss of dignity (79.3%). Assisted suicide is not really about pain or fear of it (24.7%), it is about fear of becoming dependent on others. That “choice” is no reason to endanger vulnerable people who will be pressured with a duty to die or open obvious pathways for abuse, neglect and abandonment of our elderly. We can do better in Connecticut with compassionate choices – such as expanded options for early hospice care, a “right to try” bill, training for doctors in cutting edge pain management and increased funding for home health and attendant care. In addition to all this, legalizing assisted suicide laws must be one of the worst solutions to aid people near the end of life. It would only be accessible for privileged people who can plan and navigate the necessary hurdles of waiting periods, second opinions, witnesses and more. Hundreds and thousands more Connecticut residents would truly be served if the state stayed focused on care, not killing.
It would be expanded.
In the spring of 2014, the Los Angeles Times editorialized that their state should adopt an assisted suicide law and extend it to children. At a Compassion & Choices’ press conference at the Connecticut State Capitol Building in February 2013, one of the speakers advocated extending any future Connecticut “aid in dying” law to the mentally incompetent. At an October 2014 event in Hartford, Compassion & Choices President, Barbara Coombs Lee stated with regard to including people with dementia and cognitive declines, that “It is an issue for another day but is no less compelling”. Compassion & Choices is the successor to The Hemlock Society. The Final Exit Network advocates suicide and euthanasia for people “when they judge the quality of their life to be unacceptable”. These statements, among others, reveal a broader, more radical agenda.
Assisted Suicide promotes the bigotry of ageism and ableism
The Family Institute of Connecticut is proud to work to oppose assisted suicide with so many diverse organizations. We have learned from them how assisted suicide is fed by ableism and ageism. To learn more about why assisted suicide is opposed by these organizations, we recommend the blogs of Not Dead Yet and Choice is An Illusion, and the websites for Patients’ Rights Action Fund and the Patients Rights Council.
Why Assisted Suicide Must Not Be Legalized
There are alternatives to assisted suicide
If the proponents of assisted suicide want our legislature to really tackle pain and comfort at the end of life, we suggest their money would be better spent introducing measures at the legislature such as increasing access to and awareness of palliative care, increasing the number of licensed nursing aids (and also increasing jobs), and better access to earlier hospice care. These bills would not be “emotional” and would be welcomed by all legislators who want to bring more comfort and dignity to people and their caregivers. And as a result, many more people would receive truly compassionate end of life care.
Connecticut ranks low on access to high quality home health care.
Connecticut ranks last in the country for length of stay for hospice care.
In 2014, the legislature passed a bill to investigate the use of Medical Orders regarding Life Sustaining Treatment or “MOLST” forms. These forms provide important information to health care providers and hospital employees about the treatment wishes of patients. Striking a balance of patient autonomy with proper treatment. The CT MOLST is a pilot program that we continue to monitor.
There has been abuse.
Advocates of assisted suicide assert that there has never been one case of abuse related to laws legalizing assisted suicide. Setting aside the inherent flaw of making such a broad assertion about a program designed and implemented by human beings, with a program as complicated and dangerous as assisted suicide, that claim is simply not supported by the facts. For a list of abuse cases that were uncovered through media reports visit http://dredf.org/public-policy/assisted-suicide/some-oregon-assisted-suicide-abuses-and-complications/.
Official reports not reliable. The official reports generated by the state of Oregon rely on self-reporting by doctors who are ideologically devoted to the success of assisted suicide. The Health Department for the state of Oregon has officially stated any report submitted by a physician “could have been a cock-and-bull story” and therefore their official reports generated by the state of Oregon cannot be used to “detect or accurately comment on issues that may be under reported.” They may not be used to fairly base a claim of no abuse or misuse.
There are many reports of abuse and misuse reported by the media and victims.
Thomas Middleton was a victim.
This doctor could not protect his patient from assisted suicide in Oregon.
The Vermont Alliance for Ethical Healthcare prepared an overview of many abuse and misuse cases from Oregon. A complete list may be found at their website. http://www.vaeh.org/resources/ We have copied a few cases and reprinted them below for your information.
Kate Cheney, 85, had terminal cancer and told her doctor she wanted assisted suicide. Concerned that she didn’t meet the required criteria for mental competence because of dementia, he declined to write the requested prescription and instead referred her to a psychiatrist as required by law. She was accompanied to the psychiatric consultation by her daughter. The psychiatrist found that Kate had a loss of short-term memory. It also appeared that her daughter had more interest in Cheney’s assisted suicide than did the patient herself. The psychiatrist wrote in his report that while the assisted suicide seemed consistent with Kate’s values, “she does not seem to be explicitly pushing for this.” He also determined that Kate did not have the “very high capacity required to weigh options about assisted suicide,” and he declined to authorize the lethal prescription.
Kate seemed to accept the psychiatrist’s verdict, but her daughter did not. Her daughter viewed the guidelines protecting her mother’s life as obstacles, and in a press interview called the guidelines a “roadblock” to Kate’s right to die and demanded that Kate’s HMO, Kaiser Permanente, provide a second opinion. This was provided by a clinical psychologist (rather than a MD-psychiatrist) who also found Kate had memory problems. The psychologist also worried about familial pressure, writing that Kate’s decision to die “may be influenced by her family’s wishes.” Still, despite these reservations, the psychologist determined that Kate was competent to kill herself and approved the writing of the lethal prescription. Sometime later, Kate went into a nursing home for a week so that her family could have some respite from care giving. After she returned home, she declared her desire to take the pills.
The safeguards failed Kate Cheney:
It is possible to circumvent the safeguards by “shopping” for an agreeable professional to write the lethal prescription.
By giving the interview, the patient’s daughter unintentionally revealed that the law does not adequately protect patients with diminished capacity from family coercion.
Did financial considerations influence the HMO director to write the prescription?
Dr. Charles Bentz, an internist in Portland, Oregon, diagnosed a malignant melanoma in a 76 year old man who had been under his care for over 10 years. Unfortunately, the cancer had already spread to his shoulder at the time of diagnosis, so it was not curable. Dr. Bentz referred this active man to both radiation oncology and medical oncology, using two methods to slow the cancer and prolong the man’s life.
When the patient finished the radiation therapy, the radiation oncologist informed Dr. Bentz that the patient was depressed due to his diminished physical stamina. At almost the same time, he finished his chemotherapy and asked his medical oncologist for a prescription so he could take his own life by suicide. The medical oncologist called Dr. Bentz asking him to act as the required second physician to confirm the diagnosis and prognosis before he wrote the prescription, saying secobarbital “works very well” and indicating he had used it many times. Dr. Bentz responded that he could not do this; the man had a documented depression and needed therapy for this. The oncologist then found another physician to render the required “second opinion” and did not refer the man back to his primary physician. Two weeks later the patient was dead from a lethal prescription.
Dr. Bentz obtained permission from the man’s family and obtained a copy of the death certificate which said death was from malignant melanoma.
The safeguards failed this patient:
His well-documented depression was not evaluated by a mental health specialist, nor was it treated.
His primary physician was excluded from helping him with his end-of-life concerns.
His oncologist falsified a public document by lying about the cause of death.
This 64 year old woman had a recurrence of her lung cancer in May 2008, 2 years after initial treatment had produced a remission. Her oncologist prescribed Tarceva (erlotinib), a once daily tablet, to slow the growth of the cancer and extend her life. Studies had shown it resulted in a 30-45% increase in life expectancy in advanced lung cancer. She was on the Oregon Health Plan (Medicaid) and was notified in May that the Plan would not cover the beneficial chemotherapy treatment, “but that it would cover palliative, or comfort, care, including, if she chose, doctor-assisted suicide”.
Randy Stroup, age 53, had advanced prostate cancer with a life expectancy of several months. He was given a prescription for mitoxantrone. This chemotherapy drug was not expected to produce a major extension of his life (“small, but measurable”), but studies had shown that it causes an increased quality of life, primarily by reducing pain. Coverage for this drug was denied by the Oregon Health Plan, but OHP told Randy that he could have coverage for “palliative, or comfort, care, including, if he chose, doctor-assisted suicide.”
Coverage by the OHP for specific services are established by its Health Services Commission. Their guideline states that they will not pay for diagnostic or curative care for the primary illness or care focused on active treatment of the primary illness which are intended to prolong life or alter disease progression for patients with <5% expected 5 year survival. Neither Barbara’s nor Randy’s prognosis fit into this guideline. But physician-assisted suicide did.
Assisted suicide is not dignified.
Assisted suicide does not guarantee dignity at the end of life. Prescription drugs can cause fearful, messy and undignified moments during a hastened death. Statistics are not kept on “aid-in-dying” failures, but there are news reports of panic stricken relatives calling 911, emergency room visits, hallucinations, vomiting and choking. A study from the Netherlands (which has far more experience than Oregon or Washington with “aid- in-dying”) reports that in at least 18 percent of reported physician-assisted suicides, doctors felt compelled to intervene and administer a lethal injection themselves because of “complications”. Proposals in Connecticut have not required a physician to be present when death-inducing drugs are administered. To what fate would we be subjecting the weakest of Connecticut citizens with the false promise of an easy death?
Legalizing Euthanasia or Assisted Suicide, the Illusion of Safeguards and Controls, Current Oncology, Apr. 2011, J. Pereira, citing Johanna H. Groenewoud et al, “Clinical Problems with the Performance of Euthanasia and Physician- Assisted Suicide in the Netherlands,” 342 New England Journal of Medicine (Feb. 24, 2000), pp. 553-555
Suicide contagion is real.
Oregon issues an annual Suicides in Oregon: Trends and Risk Factors report. According to the 2012 report, after decreasing in the 90s, Oregon’s suicide rate has increased to 41% above the national average. Laws such as Oregon’s Death with Dignity Act portray suicide as a reasonable means to solve a problem and vulnerable people in that state appear to be viewing suicide the same way. We should not be exalting suicide as the ultimate form of expressing one’s “choice”.
Oregon’s report was also cited in the Connecticut Office of Legislative Research Report, December 13, 2013.
The sociological phenomenon “suicide contagion” has been documented and cautioned against by the US Federal Gov’t. From the report . . “If suicide is presented as an effective means for accomplishing specific ends, it may be perceived by a potentially suicidal person as an attractive solution.” and “Such actions may contribute to suicide contagion by suggesting to susceptible persons that society is honoring the suicidal behavior of the deceased person, rather than mourning the person’s death.” Suicide Contagion and the Reporting of Suicide: Recommendations from a National Workshop, CDC, April 22, 1994. (Citation)
Out-of-state funded proponents have placed their slick advertisements promoting suicide as an solution to problems at the Connecticut state Capitol. We question the effectiveness of such ads, but more importantly note that thousands of school children pass through the corridor of the Legislative Office Building each year. These campaigns have been denounced by anti-suicide organizations such as the International Association of Suicide Prevention as “irresponsible and downright dangerous; it is the equivalent of handing a gun to someone who is suicidal”. We discourage our state legislators from permitting ads promoting illegal activity and suicide as a way for self-empowerment and problem solving.
Assisted Suicide causes anxiety.
Assisted Suicide is not a silver bullet to eliminate pain in CT. In fact, assisted suicide has not been proven to alleviate suffering at the end of life – it likely causes more anxiety, distress and eliminates choices at the end of life.
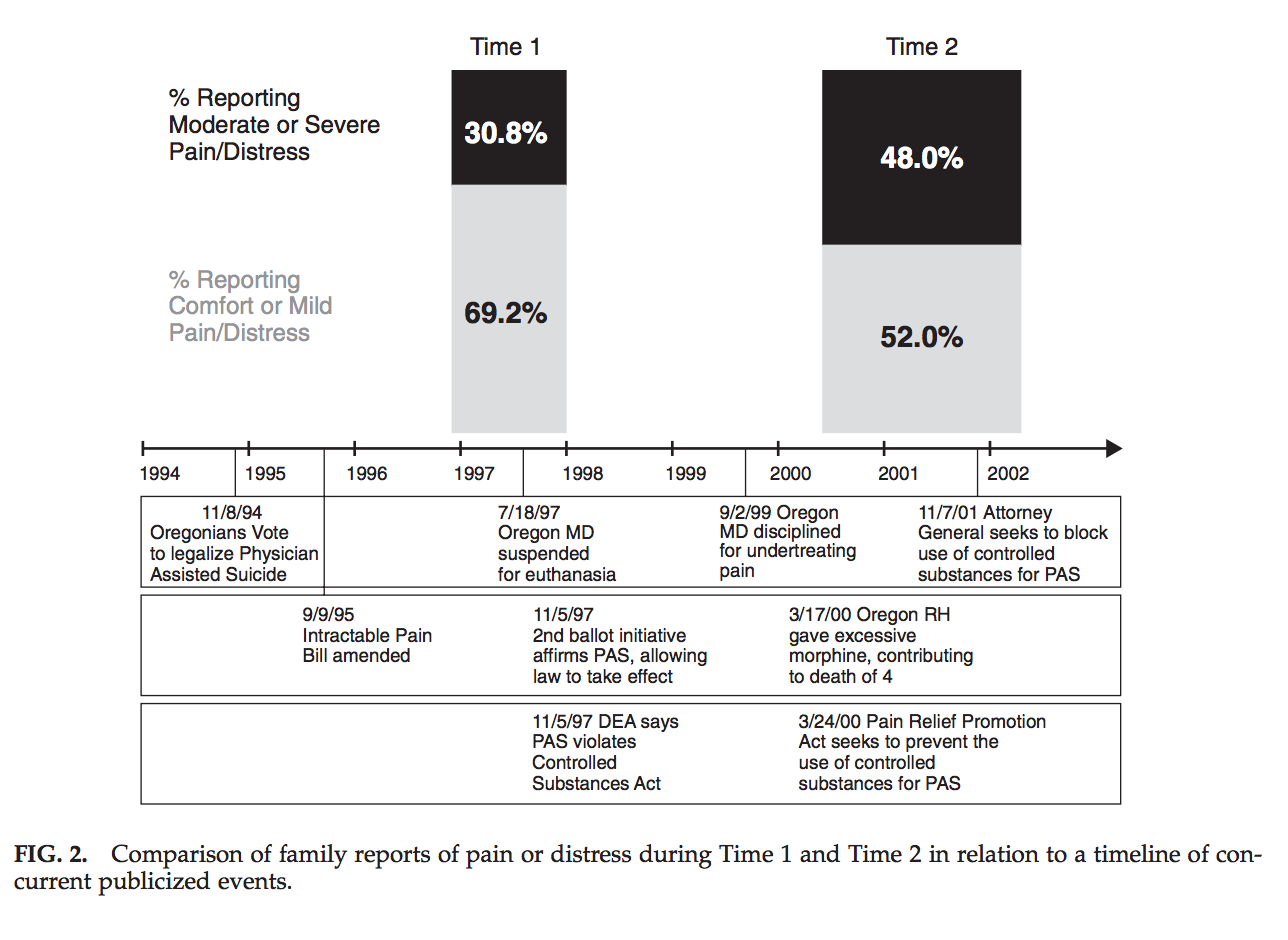
One study showed reports of pain at the end of life actually increased in Oregon from 1997 to 2002. Increased Family Reports of Pain or Distress in Dying Oregonians: 1996 to 2002, Journal of Palliative Medicine, Vol. 7, No. 3 (2004).
The last days of polka.
When people set an artificial date for their death, there is a natural risk of coercion from raised expectations by family members, friends and acquaintances. Take the case of Brittany Maynard, or a woman previously exploited by Compassion & Choices, Lovefle Svart who stated “I’d like to go on partying.” when responding to an agent of Compassion & Choices who danced with her at her “exit party”. Don Coburn, Last day of life all planned out, down to the polka, October 26, 2001 available at
http://seattletimes.com/html/localnews/2003918100_suicide02.html and analysis by Margaret Dore, http://choiceisanillusion.files.wordpress.com/2014/06/nj-a2270-legal-analysis_001.pdf
From Margaret Dore’s analysis . . “Witnesses can also be coercive. Consider Oregon resident Lovefle Svart, who threw herself an ‘exit party’ during which she danced the polka with George Eighmey of Compassion & Choices. The party was reported in the newspaper which wrote an article implying that she was in control. At the end of the party, however, when it was time for her to die, the paper also reported this exchange between her and Eighmey, which took place in front of ten people:
‘Is this what You want?’
‘Actually, I’d like to go on partying,’ Lovelle replied, laughing before turning serious
‘But, Yes.’
‘If you do take it, You will die.’ ‘Yes.’
The situation is similar to a wedding when it’s time to take your vows. Everyone’s watching and it’s the thing to do. So even if you are having second thoughts or would rather ‘go on partying’ you go forward to take the lethal dose. If Eighmey had actually wanted to give her an out, he could have said: ‘You are having so much fun, you don’t have to do this today or even next week.’ Instead, he proceeded according to the script that she would die at the end of the party. His role was to preside over her death. Her role was to comply. Once she was in this role, she no longer had control. The situation was inherently coercive.”
Expansion is only natural.
The Connecticut Legislature should consider the extension of “aid in dying” practices in Belgium and The Netherlands to twin brothers who suffered from glaucoma and back pain and to a person euthanized because they suffered a botched operation. “Loss of fitness” is now considered an underlying condition for cases worthy of euthanasia.
In 2015, an elderly couple plans to jointly commit suicide by lethal injection so their children will not be “burdened” by having to care for only one aging parent. The Connecticut Legislature must consider the true long term cost of legalizing assisted suicide.
In a March 3, 2015 letter to the editor, Connecticut doctor, Linda Alexander advocated providing “any treatment” to “all who request it” – this encompasses euthanasia on demand. Her letter is an example of why the Connecticut State Medical Society opposes physician assisted suicide. With a license from the state, many medical personnel will be unable to avoid the temptation of social expansion of assisted suicide to people outside of the “carefully” selected categories. For more information on this phenomena, consult this academic article: Legalizing Euthanasia or Assisted Suicide, the Illusion of Safeguards and Controls.
The Patients Rights Council: Addressing euthanasia, assisted suicide, advance directives, diability rights, pain control, and more.
http://www.patientsrightscouncil.org/site/
http://www.dailymail.co.uk/news/article-2262630/Brother-deaf-Belgian-twins-killed-euthanasia-describes-final-words-reveals-live-learning-going-blind.html
http://www.telegraph.co.uk/news/worldnews/europe/belgium/10346616/Belgian-killed-by-euthanasia-after-a-botched-sex-change-operation.html
2014 Position Statement by CMF New Zealand, Euthanasia and Physician Assisted Suicide.
http://www.cmf.net.nz/about-us/76-position-statement-euthanasia-and-physician-assisted-suicide
http://www.firstthings.com/web-exclusives/2014/10/lethal-ageism
Response to LA Times editorial by American College of Pediatricians.
http://www.acpeds.org/physicians-are-healers-not-killers
Assisted Death and the Slippery Slope, M.J. Shariff, Current Oncology, Jun 2012; 19(3): 143–154. http://www.ncbi.nlm.nih.gov/pmc/articles/PMC3364764/
Testimony of Peter Wolfgang, Executive Director of Family Institute of Connecticut against HB 5326, 2014’s assisted suicide bill.
http://www.cga.ct.gov/2014/PHdata/Tmy/2014HB-05326-R000317-Peter%20Wolfgang,%20Family%20Institute%20of%20CT%20-TMY.PDF
Connecticut residents like Maggie Karner, Cathy Ludlum and Elaine Kolb oppose assisted suicide and have publicly rebuked these bills and repeated attempts to pass it in Connecticut.
CONNECTICUT CITIZENS OPPOSE ASSISTED SUICIDE
The latest professional poll of Connecticut residents, the only poll dedicated exclusively to the issue of physician assisted suicide, shows that residents overwhelmingly disapprove of physicians prescribing fatal drugs for patients. Even without accurately referring to the issue as “assisted suicide”, the poll still found…
A majority of Connecticut residents (55%) believe doctors should not be allowed to prescribe or administer fatal drugs. Additionally, only 21% believe doctors should be allowed to assist a patient in taking their own life.
Click below to see the poll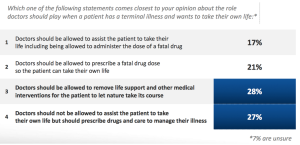
ASSISTED SUICIDE ENDS THE PATIENT, NOT THE PAIN.
Spending money yet losing momentum
After spending over $425,000 in two years, the out-of-state lobbying group that agitates for assisted suicide laws in Connecticut has had their discussion and lost repeatedly. In court, in 2009, 2013 and again in 2014 by failing to even have their bill scheduled for a vote in the Public Health Committee. In fact, notwithstanding being funded by George Soros, Compassion & Choices has dramatically decreased their level of spending in Connecticut in 2015 showing that the issue has failed in this state despite their enormous effort. Their spokesperson declared in a January 6, 2015 interview that “It appears that the electorate doesn’t care that much about it, no matter what the polling says.” The Connecticut electorate knows they would be better served by expanded access to early palliative and hospice care, increased funding for home health care workers and mandatory training for pain management techniques for medical students. These would be ways to help hundreds and thousands of Connecticut residents in ways that laws permitting assisted suicide cannot.